Artikelen
Artikelen - Mucocutane afwijkingen bij doelgerichte en immunotherapie (2019-03)
Y.S. Elshot, D. Tio, M.B. Crijns, M.W. Bekkenk
De term ‘oncodermatologie’ is overgewaaid vanuit de Verenigde Staten en heeft betrekking op diagnostiek en behandeling van dermatologische problematiek rondom de oncologiepatiënt. Ondertussen zijn er al meer dan vijftig dermatologische beelden beschreven die voorafgaand aan de diagnose (paraneoplastische dermatosen), tijdens de behandeling (cytostatica) of na de behandeling (cutane metastasen, graft-versus-host disease) kunnen optreden. De klassieke bijwerkingen van cytostatica zijn al langer bekend, maar sinds de komst van doelgerichte en immunotherapie is de hoeveelheid dermatologische bijwerkingen significant toegenomen (figuur 1 en 2).
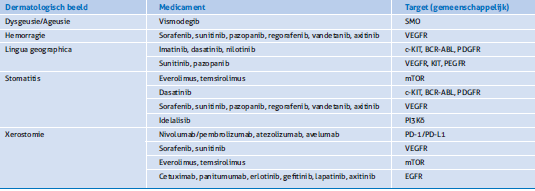
Door de grote hoeveelheid bijwerkingen hebben we ervoor gekozen in tabelvorm een overzicht te presenteren (tabel 1-3). Tijdens de Dermatologendagen wordt een aantal dermatologische beelden verder toegelicht.
Traditionele cytostatica remmen de celdeling en vertonen klassieke cytotoxische bijwerkingen zoals toxisch erytheem van chemotherapie, mucositis, extravasale schade, nagelafwijkingen en het anageen effluvium. Sinds de komst van met name de doelgerichte, maar ook de immunotherapie, zijn de hoeveelheid mogelijke mucocutane bijwerkingen significant toegenomen. Deze nieuwe therapieën trachten de groei van kankercellen te remmen door in te grijpen op specifieke signaal pathways, die betrokken zijn bij de groei en overleving van maligne cellen.
Bij doelgerichte therapie zijn de bijwerkingen direct het gevolg van de farmacologische werking van het middel gezien de moleculaire aangrijpingspunten ook in de huid en slijmvliezen aanwezig kunnen zijn.
In het geval van immunotherapie betreft het meestal bijwerkingen die secundair zijn aan de modulatie van het immuunsysteem. Bij beide, doelgerichte en immunotherapieën, is er zelden sprake van een immunologisch gemedieerde allergische reactie. Multidisciplinaire samenwerking is in het belang van de patiënt aangezien deze bijwerkingen, naast het negatieve effect op de kwaliteit van leven, bepalend kunnen zijn bij het al dan niet voortzetten van de oncologische behandeling.

Figuur 1. Pembrolizumab (anti-PD-L1) geïnduceerd bulleus pemfigoid.

Figuur 2. Woodlamponderzoek van imatinib (multikinase, waaronder C-kit, inhibitor) geïnduceerde depigmentatie.
Tabel 1. Cutane afwijkingen.
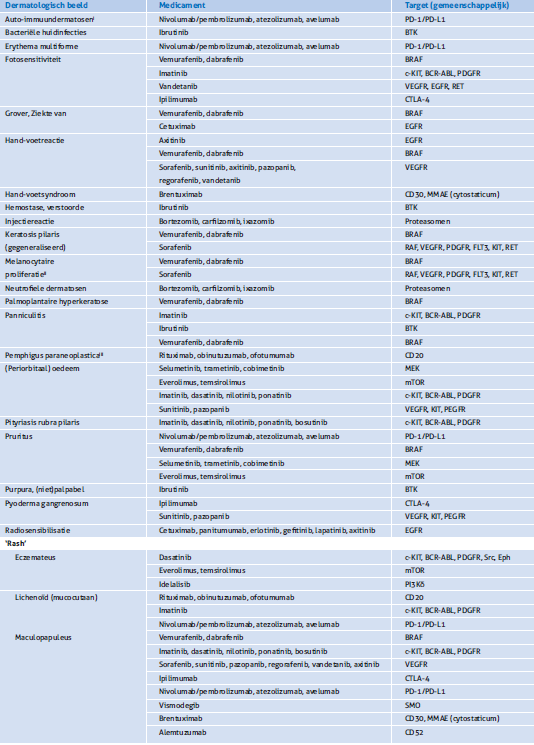
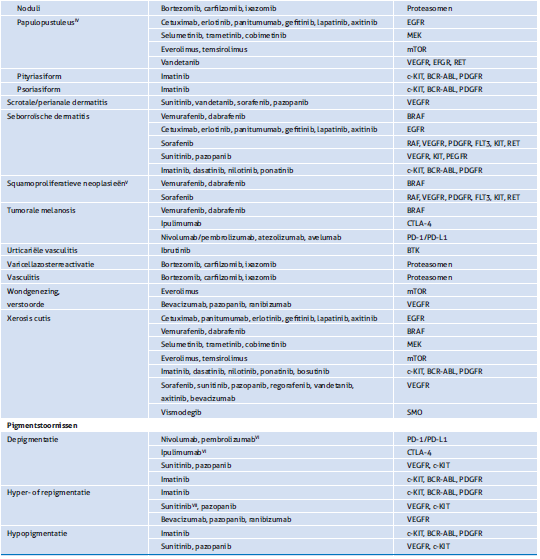
I: Bulleus pemfigoïd, dermatomyositis, sarcoïdose, alopecia areata, psoriasis (arthropathica)
II: Toegenomen pigmentatie, eruptieve naevi, regressie van naevi
III: Directe immunofluorescentie negatief
IV: Pruritus/branderigheid, impetiginisatie
V: Benigne hyperkeratotische neoplasieen, keratoacanthoom, plaveiselcelcarcinoom
VI: Wordt alleen gezien in het kader van melanoombehandeling
VII: Bruin tot grijze, maar ook (reversibele) gele verkleuring t.g.v. metabolieten
Tabel 2. Mucosale afwijkingen.
Tabel 3. Haar- en nagelafwijkingen.
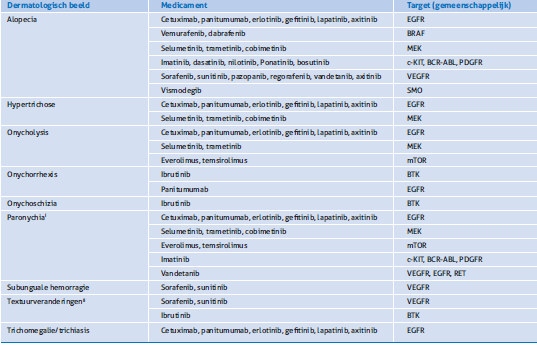
I: Primair inflammatoir met secundair impetiginisatie/granuloma pyogenicum
II: Inclusief (ont)krullen van het haar
Tabel 4. ‘Serious adverse events’

AGEP: acuut gegeneraliseerde exanthemateuze pustulosis; DRESS: drug rash with eosinophilia and systemic symptoms; DIHS: drug-induced hypersensitivity syndrome; SJS: Stevens-Johnson syndroom; TEN: toxisch epidermale necrolyse
Sinds de komst van doelgerichte en immunotherapie is de hoeveelheid dermatologische bijwerkingen van cytostatica significant toegenomen.
Literatuur
- Reyes-Habito CM, Roh EK. Cutaneous reactions to chemotherapeutic drugs and targeted therapy for cancer: Part II. Targeted therapy. J Am Acad Dermatol 2014;71(2):217.e1-217.e11.
- Macdonald JB, Macdonald B, Golitz LE, LoRusso P, Sekulic A. Cutaneous adverse effects of targeted therapies: Part I: Inhibitors of the cellular membrane. J Am Acad Dermatol 2015;72(2):203-18.
- Macdonald JB, Macdonald B, Golitz LE, LoRusso P, Sekulic A. Cutaneous adverse effects of targeted therapies: Part II: Inhibitors of intracellular molecular signaling pathways. J Am Acad Dermatol 2015;72(2):221-36.
- Peuvrel L, Dréno B. Dermatological toxicity associated with targeted therapies in cancer: optimal management. Am J Clin Dermatol 2014;15(5):425-44.
- Ransohoff JD, Kwong BY. Cutaneous adverse events of targeted thera- pies for hematolymphoid malignancies. Clin Lymphoma Myeloma Leuk 2017;17(12):834-51.
- Lacouture M, Sibaud V. Toxic side effects of targeted therapies and immunotherapies affecting the skin, oral mucosa, hair, and nails. Am J Clin Dermatol 2018;19(Suppl 1):31-9.
- Curry JL, Tetzlaff MT, Nagarajan P, Drucker C, Diab A, Hymes SR. Diverse types of dermatologic toxicities from immune checkpoint blockade therapy. J Cutan Pathol 2017;44(2):158-76.
- Sibaud V. Dermatologic reactions to immune checkpoint inhibitors: Skin toxicities and immunotherapy. Am J Clin Dermatol 2018;19(3):345-61.
- Chen CB, Wu MY, Ng CY, Lu CW, Wu J, Kao PH. Severe cutaneous adverse reactions induced by targeted anticancer therapies and immunotherapies. Cancer Manag Res 2018;10:1259-73.
Summary
Oncodermatology is the dermatologic field aimed at the dermatologic health in cancer patients. Due to rapid devel- opments in cancer treatment there are now over 50 described dermatologic side effects. Moreover, dermatologists will also be confronted with other dermatological problems like paraneoplastic syndromes, cutaneous metastases and graft-versus-host disease.
Traditional cytostatic treatment is aimed at inhibiting cell division (mitosis) and can result in cytotoxic side effect like toxic erythema of chemotherapy, mucositis, extravasation injuries, nail disorders, and alopecia. Following the arrival of targeted therapies, and to a lesser extend immune checkpoint inhibitors, a significant amount of new mucocutaneous side-effects have been described. These new agents block the growth of cancer cells by inhibiting speci- fic molecules involved in tumor pathogenesis pathways.
The side effects of targeted therapy are the direct result of the pharmacological drug effects, as the molecular targets are also present in the mucosal and cutaneous tissues.
In the case of immune checkpoint inhibitors, most are immunological side effects secondary to immune system modulation. In both types of cancer treatments, true immunological allergic reactions are rare. A multidisciplinary approach to these dermatological side effects is important as they could potentially influence the continuation of the cancer treatment, in addition to having a significant effect on the patient’s quality of life. Due to the extensive amount of side effect we have opted to presenting you with an overview, of which a selected few will be given further attention during the ‘Dermatologendagen’ of the Dutch Society of Dermatology and Venerology.
Correspondentieadres
Yannick Elshot
E-mail: y.elshot@vumc.nl